What is Hepatoblastoma?
Hepatoblastoma (HB) is a liver tumor commonly seen in children below 3 years of age.It is the third most common intra-abdominal tumor in children after Neuroblastoma and Wilm’s tumour and it accounts for 80% of the malignant liver tumours in children. It is usually diagnosed during the first 3 years of life. Extremely premature babies with a birth weight of less than a kilo has been reported to have an increased risk of HB.
Symptoms of Hepatoblastoma
The most common symptom is abdominal distension or swelling, noticed by parents or paediatrician or there may be associated vomiting and loss of appetite, poor weight gain and pain abdomen in case of advanced disease.
Diagnosis of Hepatoblastoma
Diagnosis is done based on four important parameters: clinical presentation, age of the child, imaging studies, serum alpha fetoprotein (AFP) and tissue diagnosis.
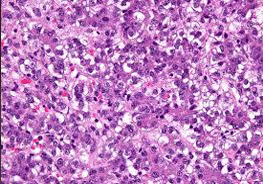
Ultrasonography remains the imaging modality of choice for primary assessment of abdominal masses.in children Magnetic Resonance Imaging (MRI) is an important modality of choice for evaluation of pediatric liver tumours. Triple phase contrast enhanced computed tomography (CECT)is another good imaging optionthat can assess arterial, venous, and portal systems. CT scan chestis doneto rule out lung metastasis. Hepatoblastomatumors frequently secrete a protein known as alpha-fetoprotein (AFP) into the bloodstream. An increase in this protein level in the blood aids in the diagnosis. A biopsy or tumor removal is used to make a final diagnosis. A biopsy is a small surgical procedure in which a small tissue from the liver tumor is taken out by a small needle under ultrasound guidance under sedation and it is examined under microscope.
Hepatoblastoma Staging and risk stratification:
PRETEXT STAGING SYSTEM: PRE-treatmentEXTent of tumor system is a pre-operative staging system based on radiological assessment at the time of diagnosis.
RISK STRATIFICATION: As per International Society of Pediatric Oncology – Liver Tumor Strategy Group (SIOPEL), there are two risk groups, standard and high risk.
| Standard risk | PRETEXT I/II/III + AFP>100ng/ml with no additional criteria |
| High risk | PRETEXT IV or any PRETEXT with AFP<100ng /ml |
Treatment for Hepatoblastoma
Hepatoblastomais treated with chemotherapy and surgery. Sometimes in higher stage disease where majority of liver is involved with tumor, liver transplantation may be required.
Chemotherapyis an important part of the treatment plan for nearly all infants and children with hepatoblastoma. Chemotherapy is used to shrink the primary liver tumor as well as to treat any hepatoblastoma that has spread outside the liver. Because cancer cells may have spread to other parts of the body, this is required for patients at all stages of the disease. These cancer cells may exist in quantities too small for Doctor to detect.
Liver transplantation has also been used successfully in conjunction with chemotherapy to treat hepatoblastoma. Liver transplants are most commonly used when the tumorhas involved three or all four segments of the liver and normal surgical resection is not possible. In these cases, the liver is completely removed and replaced with a donor's liver. Chemotherapy, like other treatments for hepatoblastoma, is used before and often after a liver transplant
RADIATION THERAPY: Radiation therapy is occasionally used in cases with positive surgical margins and in non-responsive non-resectable HB as palliation
ALTERNATIVE THERAPY: The most promising alternative approach is hepatic artery chemoembolization (HACE). Indicated in non-resectable tumors after neo-adjuvant chemotherapy, as a bridge to liver transplantation and as a palliative treatment in children with non-resectable tumors, who are unfit forliver transplantation.
For enquiries, bookings or support, call us at +91-96508 06846
Need help? Get a call back from our support team
Contact Us
