Hodgkin’s Lymphoma
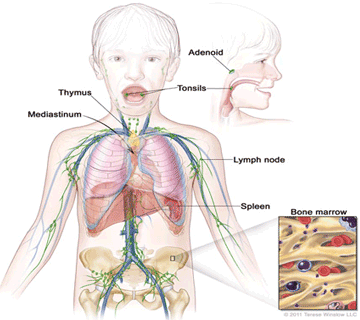
Hodgkin’s Lymphoma (HL), is a type of cancer which affects the lymph nodes in our body. The disease can spread to lungs, bones, spleen and bone marrow. It accounts for 5-7% of childhood cancers. It is more common in younger children & adolescent, young adults and older people. Almost 85-90% cases are curable with present day treatment.
What is the cause?
- Infections: Epstein Barr virus (EBV)infection can increase the risk of Hodgkin’s lymphoma. EBV DNA can be detected in 90% of HL patients in developing countries,
- Genetic Predisposition: Familial HL accounts for 4.5% of cases
- Immune dysregulation: Increased risk of HL in patients with HIV, congenital immune deficiency
- Environmental factors
What are the symptoms and signs?
Usually presents as neck swelling (enlarged neck gland) or swelling in the arm pit. There can be associated symptoms like prolonged fever or weight loss or night sweats. Liver or spleen can be enlarged. If lymph nodes inside the chest are enlarged then child will have prolonged cough or breathing difficulty and abdominal lymph node enlargement can cause pain abdomen, loss of appetite, weight loss etc.
Diagnosis
Lymph node biopsy: HL is diagnosed with a lymph node biopsy. The whole affected lymph node is excised by excision biopsy and it is examined under microscope and a special test called immunohistochemistry (IHC) done to confirm the type of HL. There are two different types of Hodgkin’s lymphoma based on biopsy report – Classical HL which accounts for almost 95% of cases and the other type is called Nodular lymphocyte predominant HL which accounts for only 5% of cases.
Other important tests are:
PET CT scan is done to look for the spread of the disease and for staging the disease. PET CT scan is done again after 2 cycles of chemotherapy to look for the response to chemotherapy
Blood investigations and 2 D echo
Bone marrow biopsy is done to look for involvement of bone marrow by HL cells in advanced stage of the disease.
Stagingand risk stratification: There are four stages of HL depending on the number and site of lymph node involvement and spread of disease to other parts of body.
- Early stage/ low risk: stage I, IIA
- Advanced stage/ high risk: IIB, III-IV (fever, weight loss , night sweats are called B symptoms)
Treatment:
Treatment is by chemotherapy. Commonly used regimen is ABVD regimen.All patients will receive chemotherapy. Low risk patients receive only 4 cycle of chemotherapy whereas high risk patients receive 6 cycles of chemotherapy
Radiation therapy is only given to patients with bulky lymph nodes (>6cm size) at the time of diagnosis and who has sub-optimal response to chemotherapy. Radiation therapy is given after completion of chemotherapy.
High dose chemotherapy with autologous hematopoietic stem cell transplantation: More than 80% of HL will get cured with normal chemotherapy and radiation therapy (if required) but in about 10-15% cases, disease can come back again specially in high risk cases, such cases are given more intensive chemotherapy followed by autologous stem cell transplantation.
Monoclonal antibodies: BrentuximabVedotin is used for high risk cases and relapse cases who are Cd 30 positive. Rituximab is used in nodular lymphocyte predominant HL
Immunotherapy is also used in relapse cases who don’t respond to conventional treatment.
For enquiries, bookings or support, call us at +91-96508 06846
Need help? Get a call back from our support team
Contact Us
